Fat Grafting 2.0: From Volume to Regeneration
Overview. Fat grafting has evolved from a simple volume-transfer technique into a sophisticated, regenerative approach for facial rejuvenation, body contouring, and reconstruction. As science improves our handling of adipose tissue, results are becoming more predictable, longer-lasting, and natural.
The Challenge with Traditional Fat Grafting
Classic fat transfer—harvest, process, inject—works, but it can be unpredictable:
Variable survival of fat cells post-transfer → need for touch-ups.
Volume loss over time, especially if integration is poor.
Complications such as fat necrosis or oil cysts when cells die during transfer.
Modern innovations aim to protect cells, enhance integration, and stimulate local regeneration so outcomes last.
Key Innovations Driving Better Results
1) Enhanced Viability Fat Transfer (EVFT)
EVFT focuses on cell protection during processing. Using agents like Poloxamer 188 (P188) to gently wash harvested fat reduces mechanical injury. In multicenter data (e.g., with the Viality system), practices report >80% retention at 12 months, versus roughly 30–40% with traditional methods.
What this means for patients: smoother contours, fewer sessions, and more durable outcomes.
2) Nanofat (Skin Quality Booster)
Nanofat is mechanically emulsified fat rich in stromal/vascular components and signaling factors, but not intended for bulk volume.
Benefits: improves texture, tone, fine lines and can support hair health by harnessing regenerative cytokines. It pairs well with microneedling, laser, or micro-coring, often shortening recovery and amplifying results.
3) Microfat + Nanofat Blending
Think structure + skin. Microfat restores three-dimensional volume (e.g., tear troughs, malar region), while nanofat refines skin quality overlying those areas.
Best for: under-eye hollowness with crepey skin, cheek shaping with luminosity gains, perioral rejuvenation.
4) AlloClae (Allogeneic Adipose-Derived Options)
For patients with limited donor fat, allogeneic adipose-derived cells/tissues can offer volume plus regenerative effects with low rejection risk and minimal downtime. These products may also be used with cellulite treatments (e.g., Aveli) to improve texture.
Note: availability and regulatory status vary by country; discuss indications, evidence, and consent in detail.
5) Fat Banking (Your “Biologic Savings Account”)
During liposuction or grafting, excess fat is processed and cryopreserved for future touch-ups or new areas—avoiding another harvest.
Who benefits: lean patients, those planning staged rejuvenation, or anyone wanting maintenance with their own tissue.
Technique Still Matters (A Lot)
Even with new tech, fundamentals drive success:
Gentle harvest/processing (avoid excessive shear or high g-forces).
Micro-parcel placement in multiple planes to maximize surface-to-capillary contact.
Slow, controlled injections to reduce cell trauma.
Meticulous patient selection and staged planning when needed.
Reported survival ranges ~25–90% depending on technique, tissue quality, and aftercare—modern methods aim to keep you near the top of that range.
Regeneration: Why Biology Changes the Game
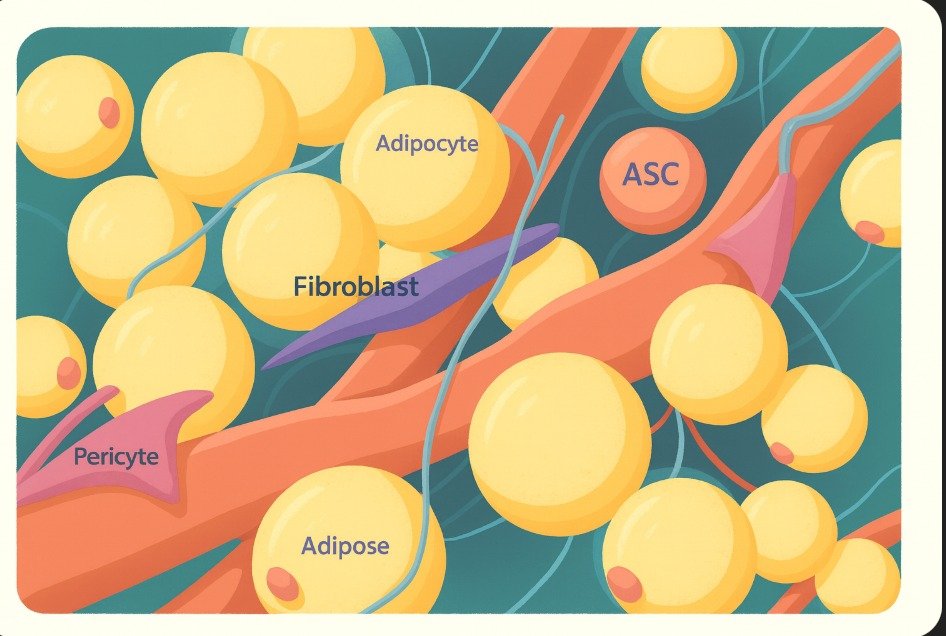
Adipose tissue carries adipose-derived stem/stromal cells (ADSCs/SVF), growth factors, and pericytes that:
Support angiogenesis (new blood supply).
Modulate inflammation and healing.
Improve dermal matrix (collagen/elasticity).
This moves fat grafting beyond filling—toward true tissue improvement.
Additives & Adjuncts (Used Judiciously)
PRP (platelet-rich plasma): concentrates growth factors; may enhance take and recovery.
Growth factors/biomaterials: under study or selectively used to stabilize grafts and guide integration (e.g., collagen scaffolds, HA matrices).
Availability, indications, and regulatory status depend on the jurisdiction and must be discussed in consent.
Safety, Ethics, and Expectations
FDA/ANVISA compliance (conforme o país) and informed consent are non-negotiable.
Be transparent about risks (irregularities, partial resorption, rare complications) and likely need for staging.
Align the plan with the patient’s goals, health, and budget; advanced biologics may increase cost.
Who Is a Good Candidate?
Volume loss of face or body, contour refinement, or skin-quality concerns.
Adequate donor fat (unless using banked or allogeneic options where permitted).
Willingness to follow aftercare and accept staged improvements for optimal longevity.
The Bottom Line
Modern fat grafting blends art + science: refined handling, regenerative biology, selective additives, and personalized planning. The result is a shift from “fill and hope” to designed integration—with outcomes that look and feel like you